Canine distemper primarily affects puppies and is caused by the canine distemper virus. Infected dogs are characterized by a biphasic fever pattern, rhinitis, severe gastrointestinal disorders, and respiratory inflammation. In later stages, neurological symptoms often develop. Various secretions and excretions—nasal discharge, saliva, tears, pericardial fluid, pleural effusion, ascites, and urine—as well as blood, cerebrospinal fluid, lymph nodes, liver, spleen, and spinal cord contain large amounts of virus and can shed the pathogen through respiratory secretions and urine. Transmission occurs via direct contact between healthy and infected dogs or through contaminated air or food entering the respiratory or digestive tract. Besides puppies, fur‑bearing species such as foxes and minks are also highly susceptible.
Diagnostic Highlights
Epidemiology
This disease peaks during the cold season (October through April), especially in areas or facilities with high dog density. Once an outbreak occurs, other puppies are almost certain to become infected unless kept in absolute isolation. Nursing puppies acquire maternal antibodies via milk and seldom develop clinical disease. Typically, puppies aged three months to one year are most vulnerable.
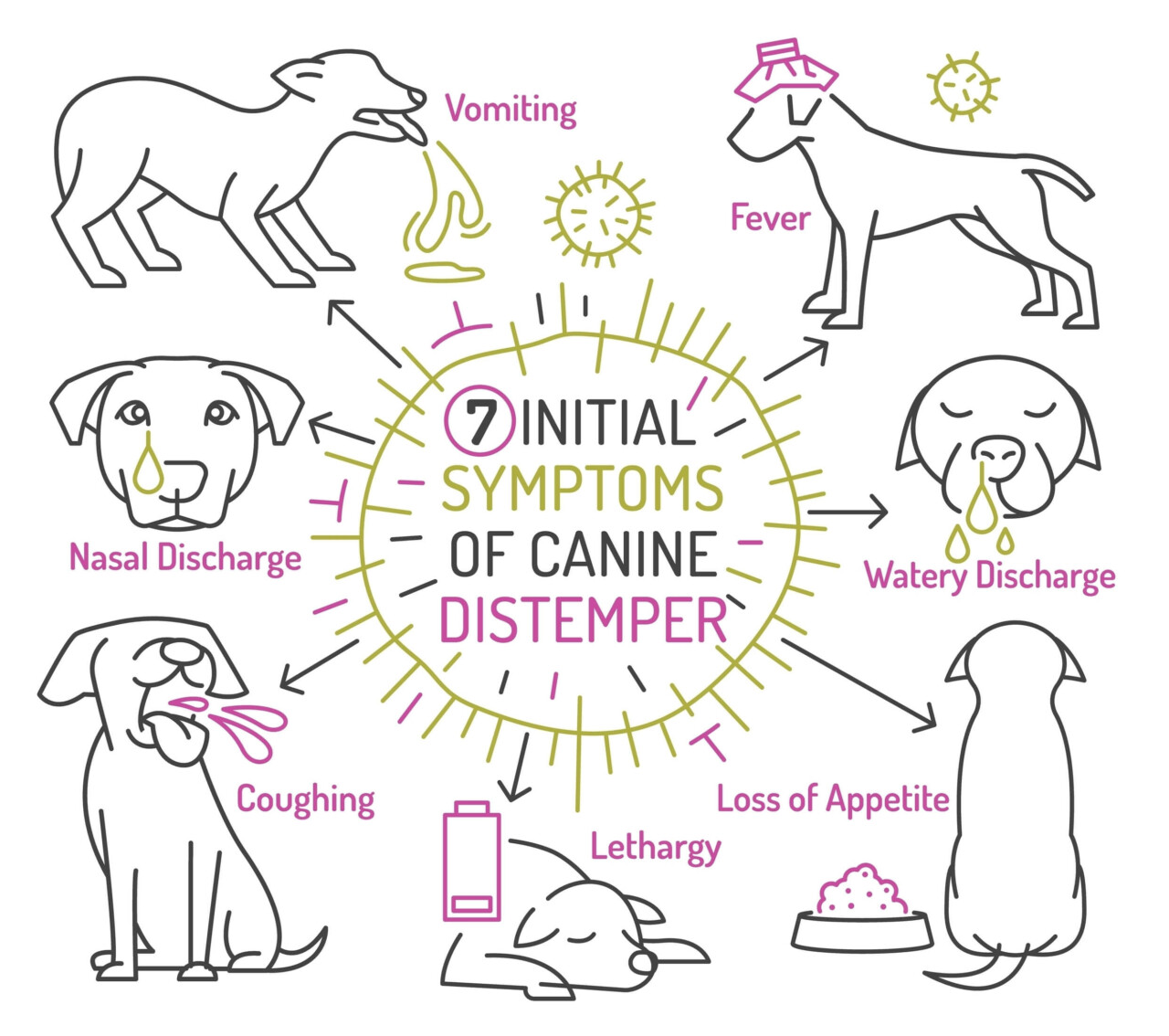
Clinical Features
The body temperature exhibits a biphasic fever pattern: it rises to approximately 40 °C for 1–2 days, returns to normal, and then elevates again after 2–3 days. During the second fever spike—when some cases may die—respiratory signs appear: coughing, sneezing, and discharge ranging from serous to purulent, with a dry nasal planum. Eyelids swell, and purulent conjunctivitis develops; corneal ulcers may follow in the later stage. On the lower abdomen and inner thighs, pinpoint erythema, edema, and purulent papules may occur. Vomiting is common; initial constipation is followed by foul‑smelling diarrhea, sometimes containing blood and gas bubbles. In rare cases, hyperkeratotic lesions may appear on the paw pads and nasal planum. Neurological symptoms may manifest at disease onset or emerge 7–10 days later.

In mild cases, local twitching of the lips and eyelids occurs; in severe cases, dogs salivate, make chewing motions, circle, collide with objects, foam at the mouth, clamp their jaws, fall and convulse in epileptiform seizures lasting seconds to minutes, with multiple daily episodes. Prognosis is generally poor. Some dogs display localized tremors or limb and hindquarter paralysis, ataxia, and other neurological deficits; even if they recover, residual weakness in the hind limbs is common.
Because canine distemper often co‑infects with canine infectious hepatitis and secondary bacterial infections complicate the clinical picture, these symptoms alone permit only a preliminary diagnosis. Definitive diagnosis requires laboratory tests—virus isolation and neutralization assays—on specimens such as conjunctival swabs, bladder fluid, gastric or pulmonary samples, tracheal washes, cerebrospinal fluid, or serum.
Prevention and Treatment
Routine Vaccination
Domestic vaccines are cell culture–attenuated. To maximize immunity, follow this schedule: first dose at six weeks of age, second at eight weeks, and third at ten weeks. Thereafter, administer one annual booster of 2 mL. Note that protective immunity develops 7–10 days post‑vaccination. Because outbreaks are common, some puppies may already be incubating the virus at the time of initial immunization and develop clinical disease under stressors such as environmental changes or long‑distance transport. To enhance protection, administer 4–5 mL of pentavalent high‑titer antiserum to newly purchased puppies, repeat after one week, and then follow the standard vaccination schedule with a pentavalent vaccine two weeks later. This approach is both safe and effective in reducing disease incidence.
Enhanced Veterinary Quarantine
Breeding facilities should practice closed herds whenever possible. During the cold season, strictly prohibit introducing outside dogs.
Prompt Isolation and Treatment
Early detection, isolation, and treatment are critical to improving cure rates and reducing mortality. In early stages, administer intramuscular or subcutaneous injections of high‑titer antiserum against canine distemper virus (or pentavalent antiserum) or convalescent canine serum. Dosage depends on disease severity and dog size, typically 5–10 mL per dose for 3–5 consecutive days. Studies report that combining antitoxin lyophilized powder injections enhances efficacy.

For antitoxin lyophilized powder, dissolve in 20 mL of sterile physiological saline or sterile water for injection and administer 2–4 vials intravenously to medium‑sized dogs; adjust dosage downward for smaller dogs. Recent data indicate that using “Canine Biokang” injectable solution in early stages, especially combined with high‑titer antiserum, yields superior results compared to monotherapy. “Canine Biokang” is dosed at 0.1–0.3 mL per kilogram body weight, intramuscularly, once or twice daily; dosage may be increased for critically ill dogs. Additionally, early use of antibiotics (e.g., penicillin, streptomycin) with symptomatic treatment is vital for preventing secondary bacterial infections and supporting recovery.
Strengthened Disinfection
Thoroughly disinfect kennels and exercise areas with appropriate disinfectants (e.g., sodium hypochlorite, phenolic agents, commercial formulations such as “Bacillol” and “Weidao” brand disinfectants).
Original article by KPTer, if reproduced, please cite the source: https://www.kaipet.com/en/common-canine-disease-diagnosis-treatment-identifying-key-symptoms-canine-distemper-common-treatment-misconceptions













Comments(2)
Very thorough! What’s the typical prognosis for dogs developing severe neurological symptoms, and what long-term support do they need?
@CriticX:Thank you for your comment! The article notes that prognosis for severe neurological symptoms from distemper is generally poor, with residual weakness common. For specific long-term support and care tailored to an affected dog, we highly recommend consulting your veterinarian.