Canine distemper, caused by the Canine Distemper Virus (CDV), is a highly contagious disease with complex clinical manifestations and a high mortality rate, ranking as the foremost infectious threat to dogs.
Etiology
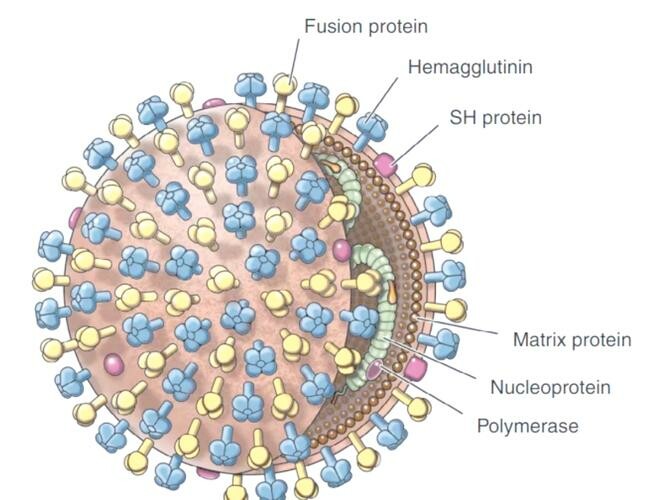
The agent, Canine Distemper Virus (CDV), belongs to the family Paramyxoviridae, genus Morbillivirus. CDV is sensitive to heat and desiccation—exposure to 50–60 °C for 30 minutes inactivates the virus. It does not survive long in hot weather, hence outbreaks most often occur in cold winter and spring months. CDV is also inactivated by ultraviolet light and alkaline solutions; in clinical practice, 3% sodium hydroxide and bleaching powder are effective disinfectants.
Epidemiology
CDV is endemic worldwide. Natural hosts include canids (dogs, wolves, jackals, foxes), mustelids (minks, skunks, weasels), and procyonids (raccoons, red pandas). Although cases can occur year‑round, incidence peaks in colder seasons. Dogs of all ages, sexes, and breeds are susceptible; however, puppies and purebreds exhibit higher susceptibility and mortality. Transmission is highly contact‑based, with infected dogs shedding virus in nasal, salivary, and lacrimal secretions, respiratory droplets, tissues, and urine. Some recovered animals may continue to shed virus and act as unnoticed carriers.
Primary transmission is via the respiratory tract, followed by the gastrointestinal route.
Pathogenesis
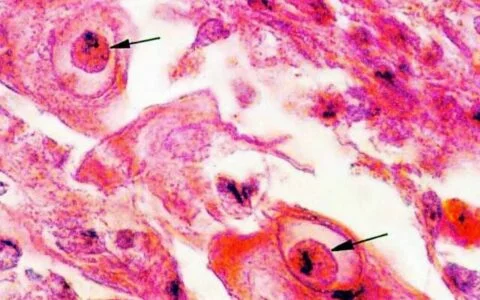
CDV’s severity stems from its pantropic nature—it infects multiple cell types and tissues. Initial infection occurs when aerosolized virus contacts the upper respiratory epithelium. Within 24 hours, the virus spreads to tonsils, retropharyngeal, and bronchial lymph nodes, causing fever and mild respiratory signs.
By days 2–4 post‑infection, extensive viral replication leads to viremia and dissemination to the liver, spleen, lungs, thymus, stomach, small intestine, and bone marrow. A second fever spike and systemic signs appear, accompanied by profound immunosuppression that predisposes to secondary bacterial and viral infections.
Around days 8–9, CDV invades epithelial and neural tissues, producing neurologic signs, nasal discharge, and hyperkeratotic lesions on the footpads.
Clinical Signs
The incubation period averages 3–6 days but varies with exposure dose. Most cases begin with respiratory signs—fever (39.5–41.0 °C), anorexia, lethargy, and serous ocular and nasal discharge. After 1–2 days, fever may subside and appetite improve, only to relapse on days 3–4 with rapid deterioration: anorexia, purulent nasal discharge, copious ocular exudate (sometimes causing corneal perforation), and pneumonia or enteritis.
In a minority of dogs, gastrointestinal signs dominate—vomiting, watery or mucoid diarrhea (occasionally hemorrhagic), severe dehydration, and wasting—mimicking canine parvovirus yet with a longer disease course of 7–10 days. Some of these dogs also exhibit mild respiratory signs.
Neurologic Manifestations
Neurologic signs can present in three patterns:
- Post‑recovery onset: 7–21 days after systemic signs subside.
- Early onset: concurrent with initial fever.
- Late onset: following severe systemic illness.
Clinical features range from focal tremors of the lips, eyelids, or a single limb to salivation, chewing motions without food, frothing, convulsions, and “staggering attacks.” Post‑ictal behaviors may include frantic barking, circling, or head‑pressing. Seizures can last seconds to minutes, occurring multiple times daily. The prognosis is often poor.
Surviving dogs may suffer sequelae—hindlimb weakness, localized muscle fasciculations, hyperkeratosis of footpads (“hard pad disease”), or nodular dermal lesions on the abdomen.
Distemper’s complex symptomatology reflects its pantropic viral nature and frequent secondary infections.
Diagnosis
Definitive virologic and serologic tests have limitations. Thus, diagnosis is usually based on epidemiologic context and characteristic clinical signs. Suspect distemper when two or more of the following occur:
- Biphasic fever: initial fever (39.5–41 °C) for 1–2 days, temporary remission, then a second fever surge on days 3–4.
- Protracted illness: poor response to symptomatic therapy—persistent cough or nasal discharge progressing to pneumonia; vomiting/diarrhea refractory to fluids and anti‑inflammatories (rule out parvovirus first).
- Bilateral conjunctivitis with mucopurulent discharge.
- Neurologic signs (tremors, seizures).
- Hyperkeratosis of footpads.
Treatment
No specific antiviral therapy exists. Management focuses on preventing secondary bacterial infections, maintaining fluid and electrolyte balance, supporting nutrition with hydrolyzed proteins, controlling fever, relieving neurologic signs, and providing sedation and antispasmodics as needed.
Successful recovery depends heavily on intensive nursing care; many affected dogs do not fully recover. While neurologic signs are often intractable, antispasmodics and sedatives can palliate symptoms.
Prevention
Immediately isolate suspected or confirmed cases. Disinfect enclosures and equipment thoroughly with 3% sodium hydroxide, bleaching powder, or veterinary‑grade disinfectants. Restrict animal movement and personnel crossings. After disinfection, maintain isolation, dryness, and optional ultraviolet irradiation for 1–2 weeks. Carcasses of deceased dogs should be incinerated or deeply buried.
Vaccination against distemper is highly effective when administered per protocol.
Recommended Vaccination Schedule
- 4–6 weeks: first dose DHPP/DHPPi (2‑in‑1)
- 7–8 weeks: first dose DHPPi/L (6‑in‑1)
- 10–12 weeks: booster DHPPi/L
- Annually thereafter: DHPPi/L booster
Original article by KPTer, if reproduced, please cite the source: https://www.kaipet.com/en/comprehensive-guide-canine-distemper-biphasic-fever-neurologic-signs-care-essentials








Comments(2)
这篇文章太全面了!我想知道,CDV 除了疫苗,还有哪些辅助预防手段吗?
@CriticX:CriticX 您好,除了疫苗,即使已接种疫苗,平时也需要加强饲养管理,给予充足且营养均衡的食物,多加锻炼,以增强它们的抵抗力。另外尽量避免带它们去到狗群密集的地方,这也很重要。谢谢您的阅读与支持!